Introduction: The escalating prevalence of multidrug resistance is a global threat to human health particularly in critically ill patients with bloodstream infections (BSIs). Delay in the administration of the appropriate antimicrobial treatment is associated with higher mortality rates and adverse consequences. This study attempted to estimate the rapid antimicrobial susceptibility testing (RAST) breakpoints directly from flagged BacT/Alert blood culture bottles in clinical practice. Material & Methods: A descriptive, cross-sectional study conducted at a tertiary care hospital in Delhi over a period of two months. The RAST was performed directly from the clinical samples for blood cultures received in our laboratory in parallel with the routine antimicrobial testing as per standard CLSI guidelines. Blood cultures were routinely incubated in BacT/Alert 3D. The inhibition zones were read at 4, 6, 8 and 16-20 hour of incubation as per European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. The identification of the isolates was confirmed by Vitek-2 compact system. Results: In our study, the area of technical uncertainty (ATU) percentage was initially high at 4 hours but decreased significantly in later incubation periods. At 4 hours, none of the S. aureus isolates showed >90% categorical agreement (CA) for any antimicrobial tested. However, clindamycin achieved the highest CA (100%) at 6 hours and 90% thereafter, with no very major errors (VME) or major error (ME). Cefoxitin required 8 hours to reach >90% CA, with no VME observed at any time point, but up to 75% ME at 8 hours. At 4 hours, most antimicrobials had high (>1.5%) rates of VME among Enterobacteriales. By 6 hours, only Meropenem and Gentamicin had >90% CA, with no VME observed for other antibiotics. Conclusion: The RAST method is relatively easy to implement in clinical microbiology labs, offering cost-effectiveness, simplicity, and rapid results, especially in resource-limited settings. However, reporting RAST results can be complex due to potential challenges with CA, VME, and ME, particularly in the initial hours of incubation and within the ATU.
| Published in | European Journal of Clinical and Biomedical Sciences (Volume 10, Issue 3) |
| DOI | 10.11648/j.ejcbs.20241003.12 |
| Page(s) | 42-50 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
RAST, EUCAST, Breakpoints, Vitek-2 Compact System, Categorical Agreement
S | ATU | R | S | ATU | R | S | ATU | R | S | ATU | R | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
S. aureus (n= 20) | 4 Hour | 6 Hour | 8 Hour | 16-20 Hour | ||||||||
Cefoxitin | 5 | 8 | 7 | 4 | 1 | 15 | 4 | 0 | 16 | 3 | 0 | 17 |
Norfloxacin | 4 | 6 | 10 | 4 | 0 | 16 | 4 | 0 | 16 | 4 | 0 | 16 |
Amikacin | 14 | 4 | 2 | 18 | 0 | 2 | 18 | 0 | 2 | 18 | 1 | 1 |
Gentamicin | 9 | 10 | 1 | 11 | 4 | 5 | 13 | 2 | 5 | 13 | 2 | 5 |
Tobramycin | 8 | 8 | 4 | 10 | 4 | 6 | 12 | 3 | 5 | 12 | 2 | 6 |
Clindamycin | 10 | 7 | 3 | 15 | 1 | 4 | 15 | 0 | 5 | 15 | 0 | 5 |
K. pneumoniae (n=10) | 4 hour | 6 hour | 8 hour | 16-20 hour | ||||||||
Amoxicillin-clavulanic acid | 0 | 6 | 4 | 1 | 3 | 6 | 1 | 2 | 7 | 0 | 0 | 10 |
Cefotaxime | 1 | 1 | 8 | 2 | 0 | 8 | 2 | 0 | 8 | 2 | 0 | 8 |
Ceftazidime | 1 | 3 | 6 | 0 | 2 | 8 | 1 | 1 | 8 | 0 | 2 | 8 |
Imipenem | 6 | 2 | 2 | 5 | 3 | 2 | 4 | 3 | 3 | 7 | 1 | 2 |
Meropenem | 2 | 2 | 6 | 1 | 1 | 8 | 1 | 1 | 8 | 1 | 1 | 8 |
Ciprofloxacin | 1 | 2 | 7 | 2 | 0 | 8 | 2 | 0 | 8 | 2 | 1 | 7 |
Levofloxacin | 0 | 2 | 8 | 1 | 1 | 8 | 1 | 1 | 8 | 1 | 1 | 8 |
Amikacin | 3 | 2 | 5 | 4 | 0 | 6 | 4 | 0 | 6 | 4 | 0 | 6 |
Gentamicin | 6 | 1 | 3 | 7 | 0 | 3 | 7 | 0 | 3 | 7 | 0 | 3 |
Tobramycin | 6 | 2 | 2 | 7 | 0 | 3 | 7 | 0 | 3 | 7 | 0 | 3 |
E. coli (n= 7) | 4 HOUR | 6 HOUR | 8 HOUR | 16-20 HOUR | ||||||||
Amoxicillin-clavulanic acid | 4 | 1 | 2 | 5 | 0 | 2 | 3 | 0 | 4 | 3 | 1 | 3 |
Cefotaxime | 4 | 1 | 2 | 4 | 1 | 2 | 4 | 1 | 2 | 5 | 0 | 2 |
Ceftazidime | 1 | 4 | 2 | 4 | 0 | 3 | 3 | 1 | 3 | 2 | 2 | 3 |
Imipenem | 5 | 1 | 1 | 6 | 1 | 0 | 6 | 1 | 0 | 6 | 1 | 0 |
Meropenem | 5 | 2 | 0 | 5 | 1 | 1 | 5 | 0 | 2 | 5 | 0 | 2 |
Ciprofloxacin | 0 | 2 | 5 | 2 | 0 | 5 | 2 | 0 | 5 | 2 | 0 | 5 |
Levofloxacin | 0 | 3 | 4 | 1 | 2 | 4 | 2 | 1 | 4 | 2 | 1 | 4 |
Amikacin | 3 | 3 | 1 | 5 | 2 | 0 | 4 | 1 | 2 | 7 | 0 | 0 |
Gentamicin | 5 | 1 | 1 | 6 | 0 | 1 | 6 | 0 | 1 | 6 | 0 | 1 |
Tobramycin | 6 | 1 | 0 | 7 | 0 | 0 | 7 | 0 | 0 | 7 | 0 | 0 |
A.baumannii (n= 3) | 4 HOUR | 6 HOUR | 8 HOUR | CLSI (Reference Method) | ||||||||
Imipenem | 1 | 0 | 2 | 1 | 0 | 2 | 1 | 0 | 2 | 0 | 0 | 3 |
Meropenem | 1 | 0 | 2 | 1 | 0 | 2 | 1 | 0 | 2 | 1 | 0 | 2 |
Ciprofloxacin | 0 | 1 | 2 | 0 | 1 | 2 | 0 | 1 | 2 | 0 | 0 | 3 |
Levofloxacin | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 0 | 3 |
Amikacin | 0 | 1 | 2 | 0 | 1 | 2 | 0 | 0 | 3 | 0 | 0 | 3 |
Gentamicin | 1 | 0 | 2 | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 0 | 3 |
Tobramycin | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 0 | 3 |
S. aureus (20) | CLSI (Reference method) | 4 Hour | 6 Hour | 8 Hour | 16-18 Hour | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
S | R | CA% | VME% | ME% | CA% | VME% | ME% | CA% | VME% | ME% | CA% | VME% | ME% | |
Cefoxitin | 16 | 4 | 61.5 | 0 | 18.8 | 89.4 | 0 | 68.8 | 90 | 0 | 75.0 | 95 | 0 | 81.3 |
Norfloxacin | 5 | 15 | 70.5 | 20 | 25 | 95 | 0 | 25 | 95 | 0 | 25 | 95 | 0 | 25 |
Gentamicin | 16 | 4 | 50 | 0 | 37.5 | 63 | 0 | 6.3 | 73.6 | 0 | 6.3 | 75 | 0 | 6.3 |
Clindamycin | 15 | 5 | 63.1 | 0 | 13.3 | 100 | 0 | 0 | 90 | 0 | 0 | 90 | 0 | 0 |
Enterobacteriales (17) | ||||||||||||||
Amoxicillin-clavulanic acid | 3 | 14 | 90 | 7.1 | 0 | 78.57 | 21.4 | 0 | 93.3 | 7.1 | 0 | 100 | 0 | 0 |
Cefotaxime | 0 | 17 | 66.6 | 29.4 | 0 | 66.60 | 35.3 | 0 | 62.5 | 35.3 | 0 | 62.5 | 41.2 | 0 |
Ceftazidime | 3 | 14 | 58.3 | 0 | 0 | 75 | 7.1 | 0 | 88.23 | 7.1 | 0 | 92.3 | 0 | 0 |
Imipenem | 7 | 10 | 42.1 | 40.0 | 0 | 69.2 | 0 | 0 | 64.28 | 30.0 | 0 | 61.53 | 60 | 0 |
Meropenem | 6 | 11 | 66.6 | 9.1 | 0 | 100 | 0 | 0 | 100 | 0 | 0 | 100 | 0 | 0 |
Ciprofloxacin | 4 | 13 | 92.3 | 23.1 | 0 | 88.8 | 0 | 0 | 88.2 | 0 | 0 | 87.5 | 0 | 0 |
Levofloxacin | 7 | 10 | 73.3 | 0 | 28.6 | 86.6 | 0 | 28.6 | 82.3 | 0 | 28.6 | 93.3 | 0 | 28.6 |
Amikacin | 5 | 12 | 61.5 | 8.3 | 0 | 57.1 | 33.3 | 0 | 68.75 | 25.0 | 0 | 52.94 | 50 | 0 |
Gentamicin | 12 | 5 | 82.3 | 0 | 0 | 94.11 | 20 | 0 | 94.11 | 0 | 0 | 94.11 | 20 | 0 |
Tobramycin | 5 | 12 | 31.2 | 58.3 | 0 | 42.1 | 0 | 0 | 47 | 75.0 | 0 | 47 | 75 | 0 |
RAST | Rapid Antimicrobial Susceptibility Testing |
CLSI | Clinical and Laboratory Standards Institute |
EUCAST | European Committee on Antimicrobial Susceptibility Testing |
AMR | Antimicrobial Resistance |
MRSA | Methicillin Resistant Staphylococcus aureus |
ICR | Inducible Clindamycin Resistance |
ESBL | Extended Spectrum Beta-Lactamase |
CRE | Carbapenem-Resistant Enterobacterales |
ATU | Area of Technical Uncertainty |
S | Susceptible |
R | Resistant |
GPC | Gram-Positive Cocci |
GNB | Gram Negative Bacilli |
CA | Categorical Agreement |
VME | Very Major Error |
ME | Major Error |
AST | Antimicrobial Susceptibility Testing |
| [1] | Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet (London, England). 2020; 395(10219): 200-11. |
| [2] | Iancu D, Moldovan I, Țilea B, Voidăzan S. Evaluating Healthcare-Associated Infections in Public Hospitals: A Cross-Sectional Study. Antibiotics. 2023 Dec 2; 12(12): 1693. |
| [3] | Evans L, Rhodes A, Alhazzani W, Antonelli M, Cooper-smith CM, French C et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med 2021; 47(11), 1181-247. |
| [4] | Marchaim D, Gottesman T, Schwartz O et al. National multicenter study of predictors and outcomes of bacteremia upon hospital admission caused by Enterobacteriaceae producing extended-spectrum b-lactamases. Antimicrob Agents Chemother 2010; 54: 5099–104. |
| [5] | EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 8.1. 2018. |
| [6] | Jonasson E, Matuschek E, Kahlmeter G. The EUCAST rapid disc diffusion method for antimicrobial susceptibility testing directly from positive blood culture bottles. J AntimicrobChemother 2020; 75: 968–78. |
| [7] | CLSI. M100Ed33. Performance standards for antimicrobial susceptibility testing: 33rd informational supplement. Wayne, PA: Clinical and Laboratory Standards Institute; 2023. |
| [8] | Ahman J, Matuschek E, Kahlmeter G. The quality of antimicrobial discs from nine manufacturers—EUCAST evaluations in 2014 and 2017. ClinMicrobiol Infect 2019; 25: 346–52. |
| [9] | Ahman J, Matuschek E, Kahlmeter G. EUCAST evaluation of 21 brands of Mueller-Hinton dehydrated media for disk diffusion testing. ClinMicrobiol Infect 2020. |
| [10] | Brown D, Canton R, Dubreuil L et al. Widespread implementation of EUCAST breakpoints for antibacterial susceptibility testing in Europe. Euro Surveill 2015; 20: 21008. |
| [11] | CLSI. M100Ed31. Performance standards for antimicrobial susceptibility testing: 31st informational supplement. Wayne, PA: Clinical and Laboratory Standards Institute; 2021. |
| [12] | Cherkaoui A, Schorderet D, Azam N, Crudeli L, Fernandez J, Renzi G, Fischer A, Schrenzel J. Fully Automated EUCAST Rapid Antimicrobial Susceptibility Testing (RAST) from Positive Blood Cultures: Diagnostic Accuracy and Implementation. Journal of Clinical Microbiology. 2022 Oct 19; 60(10): e00898-22. |
| [13] | Soo YT, Waled SN, Ng S, Peh YH, Chew KL. Evaluation of EUCAST rapid antimicrobial susceptibility testing (RAST) directly from blood culture bottles. European Journal of Clinical Microbiology & Infectious Diseases. 2020 May; 39: 993-8. |
| [14] | Heather CS, Maley M (2018) Automated direct screening for resis- tance of gram-negative blood cultures using the BD KiestraWorkCell. Eur J ClinMicrobiol Infect Dis 37(1): 117–125. |
| [15] | Park JM, Kwon M, Hong KH, Lee H, Yong D. European Committee on Antimicrobial Susceptibility Testing-Recommended Rapid Antimicrobial Susceptibility Testing of Escherichia coli, Klebsiellapneumoniae, and Staphylococcus aureus From Positive Blood Culture Bottles. Annals of Laboratory Medicine. 2023 Sep 1; 43(5): 443-50. |
| [16] | Mancini S, Bodendoerfer E, Kolensnik-Goldmann N, Herren S, Röthlin K, Courvalin P, Böttger EC. Evaluation of standardized automated rapid antimicrobial susceptibility testing of Enterobacterales-containing blood cultures: a proof-of-principle study. Journal of Antimicrobial Chemotherapy. 2020 Nov; 75(11): 3218-29. |
APA Style
Gangar, S., Nirmal, K., Lakra, A. K., Swain, K., Das, S. (2024). Clinical Practice: Estimating the Breakpoints for EUCAST Fast Antimicrobial Susceptibility Testing Using Flagged BacT/Alert Blood Culture Bottles. European Journal of Clinical and Biomedical Sciences, 10(3), 42-50. https://doi.org/10.11648/j.ejcbs.20241003.12
ACS Style
Gangar, S.; Nirmal, K.; Lakra, A. K.; Swain, K.; Das, S. Clinical Practice: Estimating the Breakpoints for EUCAST Fast Antimicrobial Susceptibility Testing Using Flagged BacT/Alert Blood Culture Bottles. Eur. J. Clin. Biomed. Sci. 2024, 10(3), 42-50. doi: 10.11648/j.ejcbs.20241003.12
AMA Style
Gangar S, Nirmal K, Lakra AK, Swain K, Das S. Clinical Practice: Estimating the Breakpoints for EUCAST Fast Antimicrobial Susceptibility Testing Using Flagged BacT/Alert Blood Culture Bottles. Eur J Clin Biomed Sci. 2024;10(3):42-50. doi: 10.11648/j.ejcbs.20241003.12
@article{10.11648/j.ejcbs.20241003.12,
author = {Seema Gangar and Kirti Nirmal and Avinash Kant Lakra and Kalyani Swain and Shukla Das},
title = {Clinical Practice: Estimating the Breakpoints for EUCAST Fast Antimicrobial Susceptibility Testing Using Flagged BacT/Alert Blood Culture Bottles},
journal = {European Journal of Clinical and Biomedical Sciences},
volume = {10},
number = {3},
pages = {42-50},
doi = {10.11648/j.ejcbs.20241003.12},
url = {https://doi.org/10.11648/j.ejcbs.20241003.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejcbs.20241003.12},
abstract = {Introduction: The escalating prevalence of multidrug resistance is a global threat to human health particularly in critically ill patients with bloodstream infections (BSIs). Delay in the administration of the appropriate antimicrobial treatment is associated with higher mortality rates and adverse consequences. This study attempted to estimate the rapid antimicrobial susceptibility testing (RAST) breakpoints directly from flagged BacT/Alert blood culture bottles in clinical practice. Material & Methods: A descriptive, cross-sectional study conducted at a tertiary care hospital in Delhi over a period of two months. The RAST was performed directly from the clinical samples for blood cultures received in our laboratory in parallel with the routine antimicrobial testing as per standard CLSI guidelines. Blood cultures were routinely incubated in BacT/Alert 3D. The inhibition zones were read at 4, 6, 8 and 16-20 hour of incubation as per European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. The identification of the isolates was confirmed by Vitek-2 compact system. Results: In our study, the area of technical uncertainty (ATU) percentage was initially high at 4 hours but decreased significantly in later incubation periods. At 4 hours, none of the S. aureus isolates showed >90% categorical agreement (CA) for any antimicrobial tested. However, clindamycin achieved the highest CA (100%) at 6 hours and 90% thereafter, with no very major errors (VME) or major error (ME). Cefoxitin required 8 hours to reach >90% CA, with no VME observed at any time point, but up to 75% ME at 8 hours. At 4 hours, most antimicrobials had high (>1.5%) rates of VME among Enterobacteriales. By 6 hours, only Meropenem and Gentamicin had >90% CA, with no VME observed for other antibiotics. Conclusion: The RAST method is relatively easy to implement in clinical microbiology labs, offering cost-effectiveness, simplicity, and rapid results, especially in resource-limited settings. However, reporting RAST results can be complex due to potential challenges with CA, VME, and ME, particularly in the initial hours of incubation and within the ATU.},
year = {2024}
}
TY - JOUR T1 - Clinical Practice: Estimating the Breakpoints for EUCAST Fast Antimicrobial Susceptibility Testing Using Flagged BacT/Alert Blood Culture Bottles AU - Seema Gangar AU - Kirti Nirmal AU - Avinash Kant Lakra AU - Kalyani Swain AU - Shukla Das Y1 - 2024/10/29 PY - 2024 N1 - https://doi.org/10.11648/j.ejcbs.20241003.12 DO - 10.11648/j.ejcbs.20241003.12 T2 - European Journal of Clinical and Biomedical Sciences JF - European Journal of Clinical and Biomedical Sciences JO - European Journal of Clinical and Biomedical Sciences SP - 42 EP - 50 PB - Science Publishing Group SN - 2575-5005 UR - https://doi.org/10.11648/j.ejcbs.20241003.12 AB - Introduction: The escalating prevalence of multidrug resistance is a global threat to human health particularly in critically ill patients with bloodstream infections (BSIs). Delay in the administration of the appropriate antimicrobial treatment is associated with higher mortality rates and adverse consequences. This study attempted to estimate the rapid antimicrobial susceptibility testing (RAST) breakpoints directly from flagged BacT/Alert blood culture bottles in clinical practice. Material & Methods: A descriptive, cross-sectional study conducted at a tertiary care hospital in Delhi over a period of two months. The RAST was performed directly from the clinical samples for blood cultures received in our laboratory in parallel with the routine antimicrobial testing as per standard CLSI guidelines. Blood cultures were routinely incubated in BacT/Alert 3D. The inhibition zones were read at 4, 6, 8 and 16-20 hour of incubation as per European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. The identification of the isolates was confirmed by Vitek-2 compact system. Results: In our study, the area of technical uncertainty (ATU) percentage was initially high at 4 hours but decreased significantly in later incubation periods. At 4 hours, none of the S. aureus isolates showed >90% categorical agreement (CA) for any antimicrobial tested. However, clindamycin achieved the highest CA (100%) at 6 hours and 90% thereafter, with no very major errors (VME) or major error (ME). Cefoxitin required 8 hours to reach >90% CA, with no VME observed at any time point, but up to 75% ME at 8 hours. At 4 hours, most antimicrobials had high (>1.5%) rates of VME among Enterobacteriales. By 6 hours, only Meropenem and Gentamicin had >90% CA, with no VME observed for other antibiotics. Conclusion: The RAST method is relatively easy to implement in clinical microbiology labs, offering cost-effectiveness, simplicity, and rapid results, especially in resource-limited settings. However, reporting RAST results can be complex due to potential challenges with CA, VME, and ME, particularly in the initial hours of incubation and within the ATU. VL - 10 IS - 3 ER -
Department of Microbiology, University College of Medical Sciences and Guru Tag Bahadur Hospital, Delhi, India
Department of Microbiology, University College of Medical Sciences and Guru Tag Bahadur Hospital, Delhi, India
Department of Microbiology, University College of Medical Sciences and Guru Tag Bahadur Hospital, Delhi, India
Department of Microbiology, University College of Medical Sciences and Guru Tag Bahadur Hospital, Delhi, India
Department of Microbiology, University College of Medical Sciences and Guru Tag Bahadur Hospital, Delhi, India
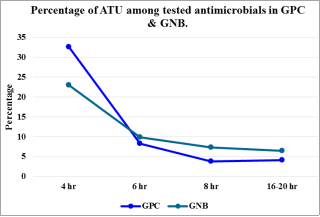
Figure 1. Percentage of ATU among tested antimicrobials in GPC and GNB at the time of reading.
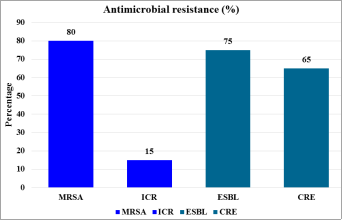
Figure 2. Distribution of antimicrobial resistance among tested isolates in the study group.

Figure 3. RAST of gram negative bacteria at 4 hour incubation (a); at 6 hour incubation (b); at 8 hour incubation (c).

